The Cataract Surgery Backlog: A Global and Regional Picture

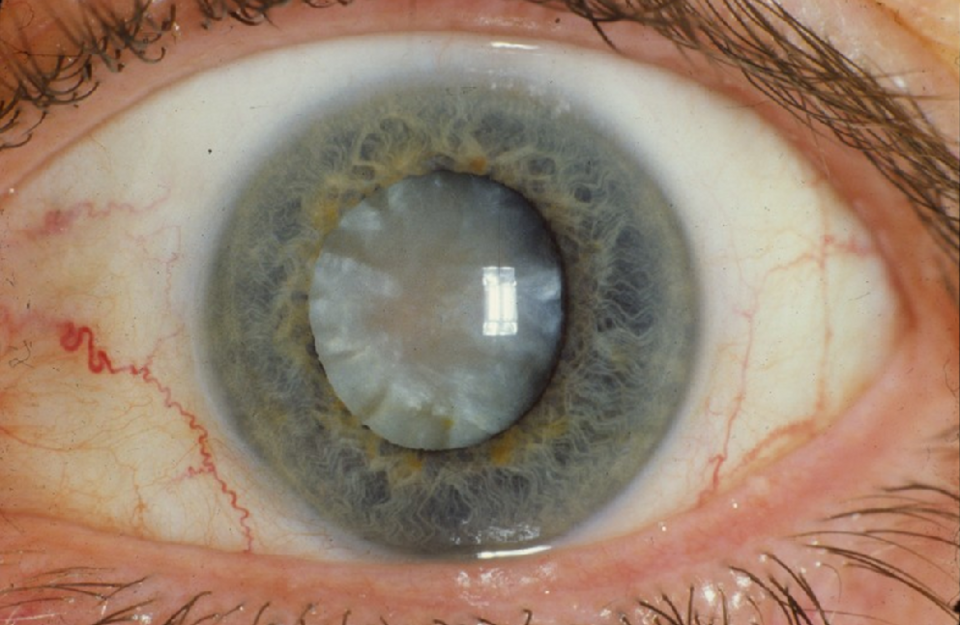
Cataracts are the world's leading cause of blindness, responsible for an estimated 17 million cases of blindness and a further 83.5 million people living with moderate to severe visual impairment globally.[1]
They are also one of medicine's more solvable problems - the surgery takes around 15 minutes, restores sight in the large majority of cases, and is consistently ranked among the most cost-effective clinical interventions in healthcare.[2] [3] Yet a major study published in The Lancet Global Health in early 2026, drawing on surveys from 68 countries, estimated that roughly one in two people who need cataract surgery worldwide still haven't received it.[4]
Understanding that gap requires looking not just at the global numbers, but at where the shortfalls are concentrated, why they persist, and who bears the heaviest burden. Crucially, the challenge is both a backlog and a flow problem. The backlog reflects the existing pool of untreated cases, while ongoing incidence adds new demand each year. Even where health systems are meeting annual demand, the backlog will only reduce if surgical capacity consistently exceeds new case formation over time.
The Scale of the Problem
Global effective cataract surgical coverage (eCSC) - a metric that accounts for both access to treatment and the quality of the outcomes - stood at an estimated 48.2% in 2025.[5] It’s clear that progress has been made, with coverage improving by around 15% over the past two decades.[6] But the pace falls well short of the WHO's target of a 30% increase by 2030, with current modelling suggesting only an 8% growth on present trends.[7]
Alongside effective coverage, cataract surgical rate (CSR) – the number of surgeries performed per million population per year, provides a complementary view of system capacity. In many low-income settings, CSR remains below 1,000, indicating severe under-capacity, while high-performing systems typically exceed 6,000. Closing the global gap requires not only improving outcomes, but materially increasing surgical throughput.
The consequences extend beyond health. Untreated visual impairment is associated with an estimated USD $411 billion in annual global productivity losses, not to mention the human cost of increased dependency, impacted mental wellbeing, and even measurably higher mortality, independent of other health factors.[8] Cataract surgery, is one of the few interventions that can restore both health and economic productivity within days. The backlog is not just a clinical problem, it is putting a profound burden on the world’s most vulnerable.
A Problem Distributed Very Unevenly
The global average breaks down into dramatic regional variation. Regardless of need, the experience of cataract and the likelihood of receiving treatment depends enormously on where you live.
Sub-Saharan Africa: The Deepest Gap
Sub-Saharan Africa has the most severe shortfall, with the WHO estimating that three in four people in Africa who need cataract surgery have not received it.[9] Individual country data is starker still - Burundi recorded an effective coverage rate of just 2.1% in 2024.[10] The primary constraint is workforce: the region has around 2.5 ophthalmologists per million people, compared to a WHO minimum of 4, and a global average of 31.7.[11] Compounding the problem further, access is concentrated in cities and leaves large rural populations without access.[12] Infrastructure gaps, weak supply chains, and low public awareness that treatment is effective exacerbate the problem.[13]
A companion study into Kenya's cataract backlog found that at current surgical capacity, an estimated 77% of people on the country's waiting list in 2025 will die before receiving surgery.[14] It's a figure that captures, perhaps more vividly than any other statistic, the reality of the issue.
South and South-East Asia: Volume Without Equity
Since the 1980s, India has made huge strides in cataract surgery volumes. The cataract surgical rate grew from around 700 operations per million people in 1981 to 6,000 per million by 2012, in large part thanks to improved efficiencies, better tools, and more adequate staffing levels.[15]
In 2022–23, under the government's Rashtriya Netra Jyoti Abhiyan campaign to clear the national cataract backlog, India performed 8.34 million cataract surgeries, exceeding its target of 7.5 million.[16] There’s also been a concerted effort to drive demand; while the figures of cataract instance are high, there are barriers to access. Social campaigns have strived to improve awareness about the safety of treatment options (and that treatment itself is even possible), as well as addressing cost barriers with free or subsidised surgeries and improved access routes.[17]
The picture is not without nuance, however; higher volumes don’t necessarily equate to better outcomes.
Baseline survey data from 2015–19 put overall cataract surgical coverage at 57.3%, but effective coverage (accounting for quality of outcome) at 36.7%, revealing a quality gap alongside the access gap that remains a focus for improvement.[18]
It’s much the same in other countries across the continent – a study in several fishing villages in Karachi found that two-thirds of the eyes that had undergone cataract surgery had some form of visual loss, and 12.4% of eyes were blind after operation. While these figures fall below the WHO recommended values, sadly they’re still relatively better than those found in a number of other studies in LMICs.[19]
Latin America, the Middle East and High-Income Markets
Latin America has made genuine progress, with rising incomes and expanding health insurance driving improved coverage in urban centres, yet rural and low socioeconomic populations remain under-served.[20] [21] The Middle East is similarly split; Gulf Arab states record figures approaching high-income country levels, while conflict-affected countries face acute shortfalls.[22]
High-income countries are not without their own pressures, though - NHS cataract waiting times increased by 84% between 2019 and 2021 as a result of the pandemic, with some London trusts reporting average waits of nearly a year from referral to surgery. [23] At the top of the Lancet study's rankings, Qatar recorded 77.7% effective coverage[24]; the contrast with Burundi's 2.1% encapsulates the full breadth of the global picture.
The Gender Gap
Globally, there’s one pattern that spans every region: gender inequality, in both cataract burden and treatment.
Women are both at a higher risk of developing cataracts than men, and less likely to receive treatment, with worse visual outcomes post-operatively if they do.[25]
This is particularly evident in developing countries and rural populations, and places where cataract outcomes remain below the goal established in the World Health Assembly 2013 Global Action Plan.[26]
The drivers are structural as much as cultural. In many lower-income settings, household healthcare spending is prioritised for, and controlled by, male family members.[27] Older women (who carry the greatest cataract burden) are more likely to be economically dependent, less mobile, and less likely to seek or be referred for treatment.[28] Fatalism compounds this: where declining sight is accepted as an inevitable part of aging, women with less autonomy over their own health decisions are the least likely to push back against it. Screening models that require patients to travel to facilities further disadvantage those with the least mobility.
Programmes that have made headway on the gender gap share common features: community-based screening that goes to patients rather than waiting for them, targeted outreach, and deliberate tracking of the gender distribution of surgeries and their outcomes. Elsewhere, the gap remains unaddressed.
The Path Forward
The tools to address the cataract backlog exist. The surgical technique is mature and effective. What has been missing is a combination of sustained funding, equitable distribution of surgical capacity, and structural attention to who is being left out. The WHO's Vision 2030 targets, national programmes in India and across Sub-Saharan Africa, and the work of non-profits like Orbis, the Fred Hollows Foundation and Sightsavers are all pulling in the right direction.[29] Whether the pace is sufficient is less clear.
What is clear is that cataract blindness remains one of the most consequential, and most preventable, public health challenges in the world. 535 million people are projected to be living with blindness or moderate-to-severe visual impairment by 2050, up from 338 million in 2020, and those untreated are concentrated almost entirely in low- and middle-income countries.[30] [31] Closing the treatment gap is both a humanitarian priority and an economic imperative. Few areas of healthcare offer such a clear, scalable opportunity to restore independence, productivity, and quality of life at population level. The question is no longer whether the problem can be solved, but whether systems can mobilise the sustained investment and capacity required to do so at scale.
Sterimedix is a UK-based manufacturer of single-use ophthalmic surgical devices, supplying ophthalmic cannulas and other devices used in cataract procedures across more than 60 countries.
Every day, our devices support thousands of cataract surgeries worldwide. In the context of a growing global backlog, the ability to deliver consistent, high-quality procedures at scale depends not only on surgical skill and infrastructure but also on the reliability and availability of core surgical instruments.
We publish regular updates on clinical and market developments in ophthalmology in our news section.
[1] National Institute for Health and Care Excellence. 2025. ‘Clinical Knowledge Summary — Cataracts’, NICE CKS <https://cks.nice.org.uk/topics/cataracts/> [accessed 2 April 2026]
[2] Adelson, Jaimie D., Rupert R. A. Bourne, Paul Svitil Briant, Seth R. Flaxman, Hugh R. B. Taylor, and others. 2021. ‘Causes of Blindness and Vision Impairment in 2020 and Trends over 30 Years, and Prevalence of Avoidable Blindness in Relation to VISION 2020: The Right to Sight: An Analysis for the Global Burden of Disease Study’, The Lancet Global Health, 9.2: e144–60 <https://doi.org/10.1016/S2214-109X(20)30489-7>
[3] World Health Organization. 2026. ‘One in Two People Facing Cataract Blindness Need Access to Life-Changing Surgery’, Who.int (World Health Organization: WHO) <https://www.who.int/news/item/11-02-2026-one-in-two-people-facing-cataract-blindness-need-access-to-life-changing-surgery> [accessed 2 April 2026]
[4] McCormick, Ian, Yamna Ouchtar, David Macleod, Anna Harte, Maria Vittoria Cicinelli, and others. 2026. ‘Effective Cataract Surgical Coverage in Adults Aged 50 Years and Older: Empirical Estimates from Population-Based Surveys in 68 Countries and Modelled Estimates for 2000–30’, The Lancet Global Health, 14.3 (Elsevier BV): e367–77 <https://doi.org/10.1016/s2214-109x(25)00435-8>
[5] McCormick, Ian, Yamna Ouchtar, David Macleod, Anna Harte, Maria Vittoria Cicinelli, and others. 2026.
[6] World Health Organization. 2026.
[7] World Health Organization. 2026.
[8] Burton, Matthew J., Jacqueline Ramke, Ana Patricia Marques, Rupert R. A. Bourne, Nathan Congdon, and others. 2021. ‘The Lancet Global Health Commission on Global Eye Health: Vision beyond 2020’, The Lancet Global Health, 9.4: e489–551 <https://doi.org/10.1016/S2214-109X(20)30488-5>
[9] World Health Organization. 2026.
[10] McCormick, Ian, Yamna Ouchtar, David Macleod, Anna Harte, Maria Vittoria Cicinelli, and others. 2026.
[11] Resnikoff, Serge, Van Charles Lansingh, Lindsey Washburn, William Felch, Tina-Marie Gauthier, and others. 2019. ‘Estimated Number of Ophthalmologists Worldwide (International Council of Ophthalmology Update): Will We Meet the Needs?’, British Journal of Ophthalmology, 104.4: bjophthalmol-2019-314336 <https://doi.org/10.1136/bjophthalmol-2019-314336>
[12] Bale, Babatunde Ismail, Marco Zeppieri, Obehi Suzan Idogen, Clinton Ifeanyi Okechukwu, Onakhe Emmanuel Ojo, and others. 2025. ‘Seeing the Unseen: The Low Treatment Rate of Eye Emergencies in Africa’, World Journal of Methodology, 15.3 (Baishideng Publishing Group Inc.) <https://doi.org/10.5662/wjm.v15.i3.102477>
[13] Bale, Babatunde Ismail, Marco Zeppieri, Obehi Suzan Idogen, Clinton Ifeanyi Okechukwu, Onakhe Emmanuel Ojo, and others. 2025.
[14] Bastawrous, Andrew, Yamna Ouchtar, Michael Gichangi, Monicah Bitok, Hillary Rono, and others. 2026. ‘Prevalence of Death in People with Vision Impairment from Cataracts before Treatment: A Case Study from Kenya’, The Lancet Healthy Longevity, 7.2: 100800 <https://doi.org/10.1016/j.lanhl.2025.100800>
[15] Murthy, Gudlavalleti VS, BK Jain, BR Shamanna, and D Subramanyam. 2014. ‘Improving Cataract Services in the Indian Context’, Community Eye Health, 27.85: 4 <https://pmc.ncbi.nlm.nih.gov/articles/PMC4069775/> [accessed 2 April 2026]
[16] Ministry of Health and Family Welfare, Government of India, ‘Rajya Sabha Unstarred Question No.1375: IMPLEMENTATION OF NPCBVI’, <https://sansad.in/getFile/annex/260/AU1375.pdf?source=pqars> [accessed 2 April 2026]
[17] Murthy, Gudlavalleti VS, BK Jain, BR Shamanna, and D Subramanyam. 2014.
[18] Gupta, Vivek, Praveen Vashist, S Sarath, Noopur Gupta, Suraj Singh Senjam, and others. 2024. ‘Effective Cataract Surgical Coverage in India: Evidence from 31 Districts’, Indian Journal of Ophthalmology, 72.Suppl 4 (Medknow): S650–57 <https://doi.org/10.4103/ijo.ijo_2835_23>
[19] Tabin, Geoffrey, Michael Chen, and Ladan Espandar. 2008. ‘Cataract Surgery for the Developing World’, Current Opinion in Ophthalmology, 19.1: 55–59 <https://doi.org/10.1097/icu.0b013e3282f154bd>, referenced in Ahmad, Khabir, Anthony B. Zwi, Daniel J. M. Tarantola, Abdul Qadeem Soomro, Rashid Baig, and others. 2015. ‘Gendered Disparities in Quality of Cataract Surgery in a Marginalised Population in Pakistan: The Karachi Marine Fishing Communities Eye and General Health Survey’, PLOS ONE, 10.7, ed. by Rohit C. Khanna: e0131774 <https://doi.org/10.1371/journal.pone.0131774>
[20] Batlle, Juan Francisco, Van Charles Lansingh, Juan Carlos Silva, Kristen Allison Eckert, and Serge Resnikoff. 2014. ‘The Cataract Situation in Latin America: Barriers to Cataract Surgery’, American Journal of Ophthalmology, 158.2: 242-250.e1 <https://doi.org/10.1016/j.ajo.2014.04.019>
[21] Hong, Hannah, Oscar J Mújica, José Anaya, Van C Lansingh, Ellery López, and others. 2016. ‘The Challenge of Universal Eye Health in Latin America: Distributive Inequality of Ophthalmologists in 14 Countries’, BMJ Open, 6.11: e012819 <https://doi.org/10.1136/bmjopen-2016-012819>
[22] Shakarchi, Fatma Shakarchi, Sila Bal, Joshua R Ehrlich, Marcia Zondervan, and Mattan Arazi. 2025. ‘Eyecare challenges in the Middle East: Priorities of a global ophthalmology task force’, Eye News <https://www.eyenews.uk.com/features/humanitarian/post/eyecare-challenges-in-the-middle-east-priorities-of-a-global-ophthalmology-task-force> [accessed 2 April 2026]
[23] Powell, Selina. 2021. ‘Waiting Times for NHS Cataract Surgery Increase 84% in England’, Aop.org.uk <https://www.aop.org.uk/ot/news/2021/10/23/waiting-times-for-nhs-cataract-surgery-increase-84-in-england> [accessed 10 April 2026]
[24] McCormick, Ian, Yamna Ouchtar, David Macleod, Anna Harte, Maria Vittoria Cicinelli, and others. 2026.
[25] Geiger, Matthew D., Alan G. Palestine, Nathan C. Grove, Karen L. Christopher, Richard S. Davidson, and others. 2024. ‘Are There Sex-Based Disparities in Cataract Surgery?’, International Journal of Ophthalmology, 17.1: 137–43 <https://doi.org/10.18240/ijo.2024.01.19>
[26] Geiger, Matthew D., Alan G. Palestine, Nathan C. Grove, Karen L. Christopher, Richard S. Davidson, and others. 2024.
[27] Kane, Sumit, Madhura Joshi, Ajay Mahal, and Barbara McPake. 2023. ‘How Social Norms and Values Shape Household Healthcare Expenditures and Resource Allocation: Insights from India’, Social Science & Medicine, 336, 116286 <https://doi.org/10.1016/j.socscimed.2023.116286>
[28] Wan, Zhongqi, Jianhao Bai, Weifang Wang, and Qing Peng. 2025. ‘Global, Regional, and National Burden of Cataract among Older Adults from 1990 to 2021: A Comprehensive Analysis Based on the Global Burden of Disease Study 2021’, Frontiers in Medicine, 12:1679828 <https://doi.org/10.3389/fmed.2025.1679828>
[29] Read more about these organisations:
Orbis - https://gbr.orbis.org/
The Fred Hollows Foundation – https://www.hollows.org/
Sightsavers - https://www.sightsavers.org/
[30] Bourne, Rupert, Jaimie D. Steinmetz, Seth Flaxman, Paul Svitil Briant, Hugh R. Taylor, and others. 2021. ‘Trends in Prevalence of Blindness and Distance and near Vision Impairment over 30 Years: An Analysis for the Global Burden of Disease Study’, The Lancet Global Health, 9.2: e130–43 <https://doi.org/10.1016/S2214-109X(20)30425-3>
[31] World Health Organization. 2023. ‘Increasing eye care interventions to address vision impairment’, Who.int (World Health Organization: WHO) < https://www.who.int/publications/m/item/increasing-eye-care-interventions-to-address-vision-impairment > [accessed 10 April 2026]